Category: Health Sciences and Medicine
CASE REPORT
Case Study on the Advancements in Diagnosis and Treatment Technologies for Military Personnel with Complex Explosive Injuries
Estudio de caso sobre los avances en las tecnologías de diagnóstico y tratamiento del personal militar con lesiones complejas causadas por explosivos
Petro Bodnar1 ![]() *
*
1L.Ya. Kovalchuk Department of Surgery No.1, Urology, Minimally Invasive Surgery I, Horbachevsky Ternopil National Medical University. Ternopil, Ukraine.
Cite as: Bodnar P. Case Study on the Advancements in Diagnosis and Treatment Technologies for Military Personnel with Complex Explosive Injuries. Salud, Ciencia y Tecnología - Serie de Conferencias. 2024; 3:1023. https://doi.org/10.56294/sctconf20241023
Submitted: 19-01-2023 Revised: 19-01-2023 Accepted: 19-01-2023 Published: 19-01-2023
Editor: Dr.
William Castillo-González ![]()
ABSTRACT
A 51-year-old military personnel with severe limb injury from mortar shelling, admitted to Orthopedic Traumatology Department, Ternopil Regional Hospital, Ukraine.
Conclusions: explosive injuries typically arise from the detonation of devices such as landmines, improvised explosive devices, or grenades, causing harm through blast, fragmentation, and thermal effects. Despite a delayed presentation to medical care, the patient underwent multiple debridement procedures, including Vacuum-Assisted Closure therapy, and vascular reconstruction, leading to limb salvage. This case underscore needs for timely medical care, addressing risks of mine blasts and cold weather injuries through training.
Keywords: Explosive Injuries; Diagnosis and Treatment; Mine Injuries; Military Personnel Health.
RESUMEN
Militar de 51 años con lesión grave en una extremidad por bombardeo de mortero, ingresado en el Departamento de Traumatología Ortopédica del Hospital Regional de Ternopil, Ucrania.
Conclusiones: las lesiones por explosivos suelen producirse por la detonación de artefactos como minas terrestres, artefactos explosivos improvisados o granadas, que causan daños por explosión, fragmentación y efectos térmicos. A pesar del retraso en la atención médica, el paciente fue sometido a múltiples procedimientos de desbridamiento, incluida la terapia de cierre asistido por vacío, y reconstrucción vascular, lo que permitió salvar la extremidad. Este caso subraya la necesidad de una atención médica oportuna, abordando los riesgos de las explosiones de minas y las lesiones por frío a través de la formación.
Palabras clave: Lesiones por Explosivos; Diagnóstico y Tratamiento ; Lesiones por Minas; Salud del Personal Militar.
INTRODUCTION
Military conflicts and warfare often result in complex injuries, presenting unique challenges for healthcare providers tasked with the diagnosis and treatment of wounded personnel. The evolving landscape of modern warfare, characterized by the use of mines and explosive devices, demands innovative approaches in both diagnosis and treatment to address the complexities associated with such injuries (1). In civilian settings, trauma surgeons may lack exposure to blast and ballistic injuries, unlike in warzones such as Ukraine, where incidents involving cluster bombs prevail. Urban hospitals in conflict areas face polytrauma from blasts and tissue cavities from ballistic injuries, highlighting the unique challenges of wartime medical care.(2,3)
In military healthcare, integrating innovative tech is crucial for diagnosing and treating complex mine injuries, considering emotional intelligence and social-psychological factors. As a particularly challenging condition, Post-Traumatic Stress Disorder (PTSD) lacks effective treatment, prompting the initiation of an exploratory clinical study to uncover the underlying mechanisms and facilitate clinical trials for treatment interventions.(4) However, responsible deployment requires careful consideration of both benefits and challenges. For example, in extended laparoscopic surgery, the combination of general anesthesia and epidural analgesia proves beneficial in managing postoperative pain.(5) The overarching goal is to ensure the safe and effective application of innovative technologies, thereby advancing the diagnosis and treatment of military personnel facing complex injuries.
Human deaths and economic damages have been caused by the continuous wars among them are Syria war, Russia-Ukraine war. To sustain military power and to influence direction of a conflict in the face of evolving battle dynamics, care must be given to protect soldiers. Technological developments in demining and IED detection are just but few examples that have recently shown the need for developing new tools for humanitarian deminers who in turn will address critical problems associated with that area.(6,7,8)
In order to treat explosive injuries efficiently, it is important to comprehend the pathophysiology and blast physics. Such injuries often lead to severe limb mutilation and hemorrhage causing soft tissue infection owing to destroyed muscles, torn fascia and microbial contamination. The high costs of landmine and unexploded ordnance detection and disposal as well as inefficiencies are a challenge. Yet with strides in deep learning, unmanned aerial vehicles, and sensing technologies, there may be hope for change that can revolutionize this area of practice mitigating human suffering in communities affected by war.(9,10,11,12) The main purpose of this case report is to outline the successes and future of integrating novel technologies in diagnosing and treating complex explosive and mine injuries among men in uniform with an emphasis on the need for war zone medicine advancement.
CASE REPORT
The patient, a 51-year-old military personnel, presented with a severe limb injury sustained during mortar shelling on the battlefield in winter time. The patient was in the Orthopedic Traumatology Department of Ternopil Regional Hospital (Ternopil, Ukraine). The injury occurred when the patient was exposed to mortar shelling in a winter battlefield setting. The left limb sustained significant damage, resulting in compromised vascular integrity. Due to the challenging circumstances of the battlefield, the patient could only receive first aid approximately 7 hours after sustaining the injury.
Upon arrival at the medical facility, the patient displayed signs of severe trauma, including extensive damage to the left limb. The affected limb showed visible deformities, swelling, and signs of ischemia. The patient reported intense pain and limited movement in the affected limb.
Throughout the presentation, the person displayed attentiveness and full cognitive awareness, registering a mental state score of 15 on the Glasgow Coma Scale. Vital indicators showed a blood pressure of 130/80 mmHg, a heart rate of 77 beats per minute, a respiratory rate of 19 breaths per minute, and oxygen saturation at 98 % (sustained with a 10 L per minute oxygen flow through a nonrebreathing mask). The individual presented with multiple injuries on the left side. (figure 1)

Figure 1. Admission (1a & 1b), Debridement Wounds (1c & 1d) and 6 days, 2 debridement wounds (1e)
He reported hearing difficulty in his right ear and tingling sensations in his left upper limb. A neurological examination revealed impaired sensory and motor functions in the affected limb. As part of the initial and follow-up assessments, we conducted radiographic and computed tomography (CT) scans, uncovering fractures in the tibia and fibula bones of the left limb. Damaged anterior and posterior tibial arteries were identified, resulting in compromised blood flow to the left limb (figure 1). Doppler ultrasound confirmed the lack of significant blood flow in these arteries. Numerous foreign body fragments were discovered in the wounds, but none had penetrated the peritoneal, pleural, or cranial cavities. Swift hospital admission ensued, initiating wound debridement. Over a span of 6 days, the patient underwent two debridement procedures, followed by three more in the subsequent 8 days. On the 10th day, a more complex approach involved four debridement procedures and the implementation of Vacuum-Assisted Closure (VAC) therapy to promote wound healing. (figure 2)
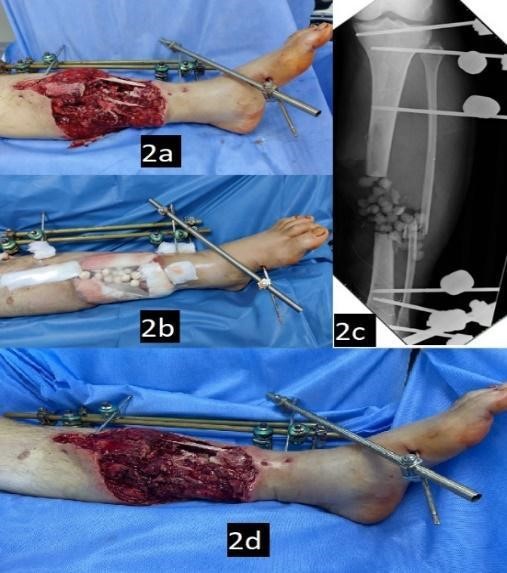
Figure 2. 8 days, 3 debridement wounds (2a, 2b & 2c), 10 days, 4 debridement wounds, VAC (2d)
A military personnel underwent vascular repair, debridement, and reconstruction using an autologous venous prosthesis and shunt. (figure 3)
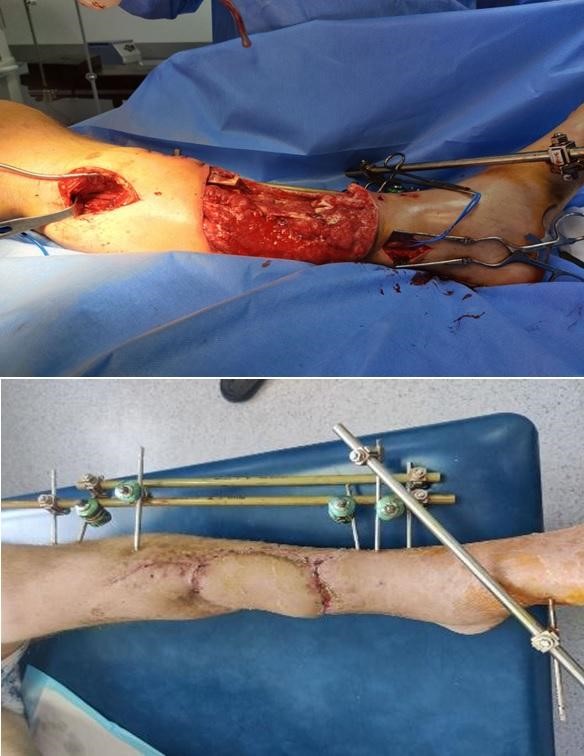
Figure 3. Popliteal-posterior-macrofibular autovenous shunting and IM Fixation
Postoperative, patient monitored closely. Adequate limb perfusion restored, antibiotics and pain management initiated. Physical therapy commenced for rehabilitation. Despite delayed presentation, vascular intervention successful, salvaging left limb. Comprehensive rehabilitation ongoing, including physical and occupational therapy, aiming for optimal functional outcomes. Regular follow-up planned to monitor vascular patency and address complications.
Timely peripheral vascular intervention and comprehensive trauma care are crucial in managing severe limb traumas. The use of autologous venous grafts and shunt to restore perfusion of the limb exemplifies the effectiveness of advanced surgical techniques in saving limbs even after long delays to surgery. This case also highlights the need for strict monitoring and early physical and occupational therapy initiation to optimize recovery outcomes. Ensuring efficient delivery of patient management using rapid, multi-disciplinary trauma care protocols that incorporate advanced wound management technologies like VAC therapy could be useful for future practice to promote survival rates as well as functional improvement among battlefield injured patients and civil victims suffering from injuries. Furthermore, on-going research efforts addressing optimal vascular repair methods and rehabilitation approaches will go a long way towards improving the quality of care regarding complex traumatic injuries. It is suggested to discuss the clinical implications of the results and how they may influence future medical practice.
DISCUSSION AND CONCLUSIONS
In winter, military personnel face risks of mine blast injuries during tactical operations and cold weather injuries like hypothermia and frostbite. These injuries cause physical and psychological trauma, particularly impacting front-line troops with increased exposure and less cold weather experience. It's important for military organizations to provide adequate training and protective equipment to mitigate the risk of these injuries during winter operations.(13)
Mine explosion injuries in military personnel commonly affect multiple body regions, particularly the feet and legs, followed by splinter-related wounds. Primary blast injuries, such as tympanic membrane rupture and blast lung damage, often result from the blast wave, causing significant physical and psychological trauma.(14,15)
Currently, there are four distinct mechanisms of harm associated with blast injury, however, a fifth mechanism has recently been hypothesized. The transmitted force and explosion overpressure comprise primary blast injuries. Debris displaced by explosion overpressure constitutes secondary blast injuries. The displacement of a victim due to blast winds and peak overpressure constitutes tertiary blast injuries. The many injuries not included in the preceding three processes are referred to as quaternary blast injuries. Quinary blast injuries are distinguished by a condition of hyperinflammation brought on by blast damage that is independent of the trauma's complexity or severity.(14) One important thing to consider was that the patient's first triage and decontamination need to happen outside of the emergency room.
Research advances in utilizing novel technologies for diagnosing and treating complex mine and explosive injuries among military personnel. The SALT triage method streamlines first responders' approach to mass casualties.(16) A novel shock-absorbing component for military vehicles has been created by researchers at the University of Maryland School of Medicine, and it may shield soldiers from blast-related brain damage. This device may increase the security of military troops who are susceptible to blast-related injuries.
Recent advancements in the military's demining and IED (improvised explosive device) detection capabilities may also be advantageous in the diagnosis and care of injured military personnel. The creation of tools and technologies that support human deminers in their job is a significant task, and demining technologies may be useful at every stage of the actual demining process.(17)
Blast injuries, once confined to military contexts, now extend to civilian settings due to IEDs in terrorist attacks. Mass casualty events demand coordinated management, necessitating detailed data on explosives, geography, victim profiles, and casualty status for risk stratification.(18) Blast exposure, common in military contexts, can lead to mental health symptoms beyond PTSD and mild traumatic brain injury. Long-term effects of blast injuries must be carefully considered. Military mine and explosive injuries pose challenges due to blast effects, shrapnel wounds, and potential limb trauma, requiring rapid diagnosis and specialized treatment. Continuous advancements in diagnostic and therapeutic methods are crucial. Worldwide, approximately 100 million land mines remain, with conflicts exacerbating casualties. A collaborative effort has yielded a remote, multisensor robotic device for detecting explosives, employing subsurface radar and imaging for precise identification, crucial in hazardous environments.(19)
The article "Mine Blast Injuries - Our Experience" details 27 mine blast cases, mostly severe with traumatic amputation and tissue contamination. Management involved frequent anesthesia-administered dressings, leading to definitive closure. Complications occurred in 26 %, but fortunately, there were no fatalities, highlighting the importance of prompt management.(20) A research paper featured in the British Journal of Ophthalmology delved into the injuries sustained by Afghan civilians involved in mine clearing operations following the Russo-Afghan war. The study detailed the nature and characteristics of these injuries, outlined the approaches taken in their treatment, explored strategies for prevention, and provided recommendations for the rehabilitation of those affected (21). In a separate investigation published in BMJ Open, the focus was on delineating the injuries inflicted upon individuals targeted by antipersonnel improvised explosive devices (AP-IEDs) and contrasting them with injuries previously outlined in studies on antipersonnel mines (APM). This study meticulously recorded injury details to elucidate patterns and characterize the nature of injuries sustained by individuals subjected to AP-IEDs.(22)
An examination conducted by DTIC, which focused on service members wounded in explosions from March 2003 to October 2006, investigated the occurrence of primary blast injuries in US military operations abroad.(23) We promptly coordinated with hospital departments upon notification, prepared for potential influx of casualties. Despite four injuries in this incident, no further admissions occurred; ensured before surgery no other blast-related casualties were admitted.
Mine blast injuries in cold weather present a grave danger to military personnel, underscoring the need for ongoing research. Discussions underscored blast injury mechanisms, advocating for innovative solutions like the SALT triage system and shock-absorbing devices. Advancements in demining tech and robotics demonstrate collaborative efforts. Timely and effective management is crucial to reduce complications and fatalities, urging continuous adaptation in diagnostic and therapeutic strategies for global conflicts.
BIBLIOGRAPHIC REFERENCES
1. Robinson A, Smith D. To clear deadly land mines, science turns to drones and machine learning. Scientific American [Internet]. [cited 2024 Jun 10]; Available from: https://www.scientificamerican.com/video/to-clear-deadly-land-mines-science-turns-to-drones-and-machine-learning/
2. Schmitt KU, Niederer PF, Cronin DS, Morrison III B, Muser MH, Walz F. Trauma Biomechanics [Internet]. Cham: Springer International Publishing; 2019. Ballistic and Blast Trauma; [cited 2024 Jun 10]; p. 247-80. Available from: https://doi.org/10.1007/978-3-030-11659-0_11
3. Maitland L, Middleton L, Veen H, Harrison DJ, Baden J, Hettiaratchy S. Analysis of 983 civilian blast and ballistic casualties and the generation of a template of injury burden: An observational study. eClinicalMedicine [Internet]. 2022 Dec [cited 2024 Jun 10];54:101676. Available from: https://doi.org/10.1016/j.eclinm.2022.101676
4. Serhiyenko V, Holzmann K, Holota S, Derkach Z, Nersesyan A, Melnyk S, et al. An exploratory study of physiological and biochemical parameters to identify simple, robust and relevant biomarkers for therapeutic interventions for ptsd: Study rationale, key elements of design and a context of war in Ukraine. Proceeding Shevchenko Sci Soc Med Sci [Internet]. 2022 Dec 30 [cited 2024 Jun 10];69(2). Available from: https://doi.org/10.25040/ntsh2022.02.14
5. Kamel IS. The role of robotics and automation in surgery: critical review of current and emerging technologies. Futur Med [Internet]. 2023 Mar 30 [cited 2024 Jun 10]:23-35. Available from: https://doi.org/10.57125/fem.2023.03.30.03
6. Syrian Revolution 12 years on | Nearly 614,000 persons killed since the onset of the revolution in March 2011 - The Syrian Observatory For Human Rights n.d. Syriahr.com. [cited 2024 Jun 10]. Available from: https://www.syriahr.com/en/291981/
7. Hu QR, Shen XY, Qian XM, Huang GY, Yuan MQ. The personal protective equipment (PPE) based on individual combat: A systematic review and trend analysis. Def Technol [Internet]. 2022 Dec [cited 2024 Jun 10]. Available from: https://doi.org/10.1016/j.dt.2022.12.007
8. 1 Introduction | Alternative Technologies to Replace Antipersonnel Landmines | The National Academies Press n.d. [cited 2024 Jun 10]. Available from: https://nap.nationalacademies.org/read/10071/chapter/3
9. Amin M, Rehman AU, Akhtar A. Antipersonnel improvised explosive device (AP-IED) blast at Muzaffarabad, AJK: orthopaedic injury profile of victims. Pakistan Armed Forces Med J. 2020;70:346-51.
10. Bosse MJ, Ficke JR, Andersen RC. Extremity war injuries: Current management and research priorities. J Am Acad Orthop Surg [Internet]. 2012;20:viii–x. Available from: http://dx.doi.org/10.5435/jaaos-20-08-viii
11. Military health and readiness improved through collaboration with small business [Internet]. DVIDS. [cited 2024 Jun 10]. Available from: https://www.dvidshub.net/news/455954/military-health-and-readiness-improved-through-collaboration-with-small-business
12. Robledo L, Carrasco M, Mery D. A survey of land mine detection technology. Int J Remote Sens [Internet]. 2009 May [cited 2024 Jun 10];30(9):2399-410. Available from: https://doi.org/10.1080/01431160802549435
13. Home- Defense Centers for Public Health - Aberdeen [Internet]. Cold Weather Casualties and Injuries- Defense Centers for Public Health - Aberdeen; [cited 2024 Jun 10]. Available from: https://ph.health.mil/topics/discond/cip/Pages/Cold-Weather-Casualties-and-Injuries.aspx
14. Shakargy JD, Gendler S, Talmy T, Shushan G, Radomislensky I, Tsur AM, Almog O, Avital G, Benov A, Gelikas S. Blast Injury Patterns Among Israel Defense Forces Fatalities. Mil Med [Internet]. 2022 Oct 7 [cited 2024 Jun 10]. Available from: https://doi.org/10.1093/milmed/usac280
15. Mathews ZR, Koyfman A. Blast Injuries. J Emerg Med [Internet]. 2015 Oct [cited 2024 Jun 10];49(4):573-87. Available from: https://doi.org/10.1016/j.jemermed.2015.03.013
16. Kujirai D, Fujii R, Kaito D, Nakama R, Izawa Y. Blast injuries by an improvised explosive device in japan: A case report. Cureus [Internet]. 2022; Available from: http://dx.doi.org/10.7759/cureus.32118
17. Lerner EB, Schwartz RB, Coule PL, Pirrallo RG. Use of SALT triage in a simulated mass-casualty incident. Prehosp Emerg Care [Internet]. 2010;14(1):21–5. Available from: http://dx.doi.org/10.3109/10903120903349812
18. Counter improvised explosive devices (C-IED) [Internet]. Dtic.mil. DEFENSE INNOVATION MARKETPLACE; 2018 [cited 2024 Jun 10]. Available from: https://defenseinnovationmarketplace.dtic.mil/communities-of-interest/counter-improvised-explosive-devices-c-ied/
19. Capineri L, Pochanin G, Bechtel T, Lande T-S, Capan I, Pastuovic Z, et al. NATO advanced research workshop on explosives detection. In: NATO Science for Peace and Security Series B: Physics and Biophysics. Dordrecht: Springer Netherlands; 2019. p. 1–32.
20. Harjai MM, Agarwal DC, Dave P, Jog SS, Arora P SM, VSM. Mine blast injuries - our experience. Med J Armed Forces India [Internet]. 2005;61(2):143–7. Available from: http://dx.doi.org/10.1016/s0377-1237(05)80010-3
21. Muzaffar W. Mine blast injuries: ocular and social aspects. Br J Ophthalmol [Internet]. 2000;84(6):626–30. Available from: http://dx.doi.org/10.1136/bjo.84.6.626
22. Smith S, Devine M, Taddeo J, McAlister VC. Injury profile suffered by targets of antipersonnel improvised explosive devices: prospective cohort study. BMJ Open [Internet]. 2017;7(7):e014697. Available from: http://dx.doi.org/10.1136/bmjopen-2016-014697
23. Ritenour AE, Blackbourne LH, Kelly JF, McLaughlin DF, Pearse LA, Holcomb JB, et al. Incidence of primary blast injury in US military overseas contingency operations: A retrospective study. Ann Surg [Internet]. 2010;251(6):1140–4. Available from: http://dx.doi.org/10.1097/sla.0b013e3181e01270
FINANCING
No financing
CONFLICT OF INTEREST
The author declare that there is no conflict of interest
AUTHORSHIP CONTRIBUTION
Conceptualization: Petro Bodnar.
Data curation: Petro Bodnar.
Formal analysis: Petro Bodnar.
Acquisition of funds: Petro Bodnar.
Research: Petro Bodnar.
Methodology: Petro Bodnar.
Project management: Petro Bodnar.
Resources: Petro Bodnar.
Software: Petro Bodnar.
Supervision: Petro Bodnar.
Validation: Petro Bodnar.
Display: Petro Bodnar.
Drafting - original draft: Petro Bodnar.
Writing - proofreading and editing: Petro Bodnar.